Coronavirus disease: COVID-19
16th March 2020
Covid-19 hits funeral industry in the pocket
24th March 202024 March 2020 | Story Keertan Dheda, Valerie Mizrahi, Digby Warner and Robert Wilkinson. Image Michael Reiche, Timothy de Wet, Ryan Dinkele and Digby Warner. Read time 10 min.
South Africa has one of the highest rates of tuberculosis (TB) infection globally. Almost 400 000 patients are treated for TB annually. It is also the most common cause of death in South Africa.
As TB researchers at the University of Cape Town (UCT) in South Africa, there is a lot we know about the disease.
We’ve been involved in understanding and intervening in HIV-associated TB, evaluating new vaccine strategies and defining how drug resistance impacts TB control in South Africa.
We’ve also used bio-markers – measurable indicators found in the body – to predict disease progression.
However, there is still a great deal we don’t know about TB. And there is still much work to be done. That includes gaining greater understanding of the bacterium’s basic biology, learning more about how it is spread from one individual to the next, and the ways it interacts with its human host at different stages of infection and disease.
As TB researchers at the University of Cape Town (UCT) in South Africa, there is a lot we know about the disease.
We’ve been involved in understanding and intervening in HIV-associated TB, evaluating new vaccine strategies and defining how drug resistance impacts TB control in South Africa.
We’ve also used bio-markers – measurable indicators found in the body – to predict disease progression.
However, there is still a great deal we don’t know about TB. And there is still much work to be done. That includes gaining greater understanding of the bacterium’s basic biology, learning more about how it is spread from one individual to the next, and the ways it interacts with its human host at different stages of infection and disease.
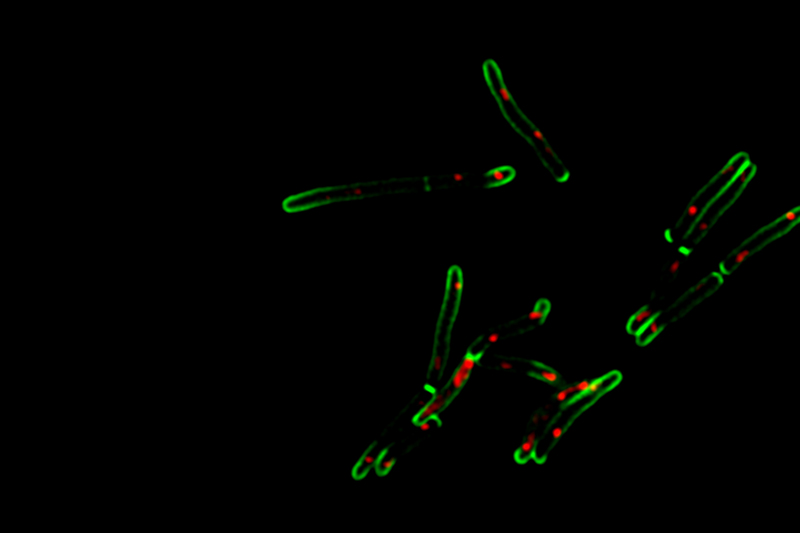
Fluorescence microscopy of mycobacteria – the green fluorescence indicates the cell wall and growth at the bacillary tips (poles) while the red fluorescence marks the position of the chromosomal DNA. Note the formation of internal walls (septa) in bacteria undergoing cell division.
It’s important to shorten the duration of TB treatmen.
Here are three things we still don’t know – and what researchers are doing to fill the knowledge gaps.The who, when, where and why of spread
The spread of TB from person to person has mostly been understood from an epidemiological point of view. This means it’s largely focused on reporting cases and identifying transmission hotspots. But when it comes to the exact mechanics of transmission, textbooks mostly rely on descriptions of how infected individuals spread the disease via aerosols generated by coughing.
The idea of bacterial aerosols has been supported by many studies. But there are still gaps in our understanding. We don’t know whether cough is necessary to produce aerosols; if infected individuals produce these droplets constantly; and how long after starting anti-TB treatment individuals stop producing them. We also don’t know whether individuals who have been infected with TB but do not show active symptoms can spread the disease.
To answer these questions, a research team from UCT and the Desmond Tutu HIV Centre, in conjunction with teams from Stanford University, Imperial College London and Massachusetts Institute of Technology (MIT), is conducting an innovative research study in Masiphumelele, an area in Cape Town hard hit by TB.
In an attempt to better understand how TB is transmitted through the air, they put patient volunteers in a sealed-off booth and collect 300 litres of the air they exhale by concentrating it into about five millilitres of liquid. Then the very difficult task of finding the TB mycobacterium (which is smaller than a blood cell) in this liquid is done by using fluorescence to light up the walls of the mycobacterial cells. This makes them easier to find.
Another UCT team has recently developed cough aerosol sampling technology which has indicated that TB bacteria from highly infectious people are genetically no different from those who are less infectious. This suggests that host pathogen interaction is likely more important than the bacterium’s genetic make up.
Our teams are looking at alternative solutions
Contrary to popular belief, they found that a substantial proportion of patients with highly drug-resistant TB – thought to have less capacity to transmit disease – were also highly infectious.How can we treat TB faster and more effectively?
It’s important to shorten the duration of TB treatment: the standard treatment regimen consists of six months of daily antibiotics. This is onerous for patients and, in the case of non-adherence, can create a window for the TB bacterium to mutate and become drug resistant.
Research into reducing the treatment time for TB takes three main approaches, all of which we are trying: identifying vulnerabilities in the TB bacterium that can be exploited by specific drugs; testing existing drugs in new combinations; and uncovering drugs that can inhibit the TB bacterium’s ability to mutate.
With the first approach, understanding the basic machinery of the TB bacterium better means scientists can exploit its weaknesses. For example, how does a TB bacterium use different carbon sources such as glucose or cholesterol to support its growth? If there is only one way, then interrupting this pathway or reaction would be a very effective way of treating TB.
There is already a slow decline of TB infections in South Africa
The second approach, trying all available drugs in all available combinations, is a common but resource-intensive strategy. Like some other scientists globally, our teams are looking at alternative solutions: for example, testing selected drug combinations in conjunction with genetics to determine which drugs have the greatest impact on the bacterium’s ability to survive.We have also been applying the third approach. It is much more complex and our work in this area has been ongoing for 16 years. It’s too early to share the details but we will soon be publishing exciting results demonstrating the concept that experimental, ‘anti-evolution’ drugs can inhibit the ‘mutating machinery’ of TB. That prolongs the utilities of existing and new anti-TB drugs.
Can we defeat TB?
While 10 million people are infected with TB around the world each year, we believe that research into TB over the next decade will yield results.
There is already a slow decline of TB infections in South Africa, likely related to improved living conditions and poverty reduction in vulnerable groups, better access to health care, and widespread roll out of antiretroviral therapy. That therapy prevents and reduces mortality in patients with HIV-associated tuberculosis.
Our institution has led the way in testing a new TB vaccine candidate dubbed M72/AS01E. During 2019, the results from preliminary medical trials – which took place at sites in South Africa, Kenya and Zambia over the course of three years – showed a 50% success rate in preventing the development of full-blown TB in young adults already infected with the disease.
Two out of every five patients globally remain undiagnosed or undetected
The trial not only provided the opportunity for researchers to better understand how the immune response can protect against TB in humans. It also showed that a vaccine can offer long-term protection. If people infected with latent TB can be offered durable protection against developing the disease, the cycle of TB transmission may be interrupted.The efficient diagnosis of TB represents a major unmet need. Two out of every five patients globally remain undiagnosed or undetected. A research team at UCT has developed a portable, battery-operated molecular TB testing strategy that detects TB DNA in sputum. Unlike the current passive case-finding approach this will take diagnostic testing from the laboratory into the community, so circumventing transmission. The university has also patented a urine test that is a much faster, simpler and cheaper way to detect TB. It is currently being developed as a community-based screening test.
This article was published in The Conversation, a collaboration between editors and academics to provide informed news analysis and commentary. Its content is free to read and republish under Creative Commons; media who would like to republish this article should do so directly from its appearance on The Conversation, using the button in the right-hand column of the webpage. UCT academics who would like to write for The Conversation should register with them; you are also welcome to find out more from [email protected].
https://www.news.uct.ac.za/news/research-office/-article/2020-03-24-tb-scientists-know-a-great-deal-but-theres-still-more-to-learn


